
INTRODUCTION
Musculoskeletal disorders affecting the upper extremities are prevalent among the general population ( Huisstede et al., 2006; Lucas et al., 2022). Individuals experiencing musculoskeletal disorders in the upper extremities often express restrictions in daily activities associated with the upper extremities ( Røe et al., 2021; van Kooij et al., 2021; Vincent et al., 2021). These limitations, as perceived by the patients, are deemed significant for their overall daily functioning ( Røe et al., 2021; van Kooij et al., 2021; Vincent et al., 2021). Considering this, it is crucial to employ a patient-reported outcome measure (PROM) to assess upper extremity function and measure the extent of limitations in these vital activities for individuals in this population. The quantification of upper extremity function using the PROM would make the assessment more relevant to patients in line with the current recommendations of patient-centered healthcare.
The upper extremity functional index (UEFI) is an upper extremity region-specific PROM commonly used to measure the extent of activity limitations caused by upper extremity disorders ( Stratford et al., 2001). The UEFI demonstrated good measurement properties ( Stratford et al., 2001; Chesworth et al., 2014), leading to the translation of the original English version to other languages and cultures ( Xiao et al., 2012; Aytar et al., 2015; Aljathlani et al., 2022; Karanasios et al., 2023). These included the translation and cultural adaptation of the UEFI into Arabic language ( Aljathlani et al., 2022). The adapted Arabic UEFI was simple and understandable to Arabic-speaking patients with upper extremity musculoskeletal disorders. Prior studies have examined the measurement properties of the Arabic UEFI in individuals with upper extremity musculoskeletal disorders and also in individuals with chronic obstructive pulmonary disease ( Alnahdi and Albarrati, 2021; Aljathlani et al., 2022; Alnahdi, 2023). These prior reports suggested that the Arabic UEFI has excellent internal consistency with homogenous items, test–retest reliability, reasonable measurement error, and substantiating evidence for its construct validity and responsiveness as a tool for assessing upper extremity function. On the other hand, these studies failed to examine the Arabic UEFI structural validity which constitutes an important and relevant measurement property for the PROM.
Structural validity is defined as “The degree to which the scores of a health-related patient-reported outcome instrument are an adequate reflection of the dimensionality of the construct to be measured” ( Mokkink et al., 2010). The UEFI was developed to assess one construct that is upper extremity function and all items seem as indicators and reflections of this construct. The structural validity of the UEFI was not formally examined in the original development of the scale by Stratford et al. (2001). To the best of our knowledge, there is only one study in the literature that examined the dimensionality and structural validity of the UEFI ( Hamilton and Chesworth, 2013). The authors used the Rasch measurement model and supported the unidimensionality of the UEFI after modification to the scale to achieve a unidimensional structure ( Hamilton and Chesworth, 2013). Given that the UEFI was developed using a reflective model where all items are reflections of one construct, it is important to formally examine this assumed unidimensionality ( de Vet et al., 2011). To date, no prior studies have examined the internal structure and dimensionality of the Arabic UEFI; thus, the structural validity of the Arabic UEFI has not been established yet and the current study is aiming to address this gap in the literature. The aim of this study was to examine the structural validity of the Arabic UEFI using both exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) in patients with upper extremity musculoskeletal disorders. We hypothesized that the Arabic UEFI would demonstrate a unidimensional structure reflecting upper extremity function. Addressing the aim of the study would allow clinicians and researchers to use the Arabic UEFI with confidence in the number of constructs measured by the scale and the validity of the scoring method.
MATERIALS AND METHODS
Study design
This study was designed as a cross-sectional study with an assessment of the participants at one time point.
Setting and participants
Participants were recruited for the current research study via convenience sampling from multiple outpatient physical therapy departments, namely the Security Forces Hospital, King Abdulaziz Medical City, and PhysioTrio Clinic, all located in Riyadh, Saudi Arabia. The research study was carried out following the rules of the Declaration of Helsinki and ethical approval was granted by the institutional review board of the Security Forces Hospital (H-01-R-069). Participants provided their consent by signing informed consent documents before taking part in the study. The criteria for inclusion in the study comprised individuals aged 18 years or older presenting with upper extremity musculoskeletal disorders. Exclusion criteria encompassed the inability to comprehend the Arabic language and the presence of disorders other than upper extremity musculoskeletal issues causing functional limitations as perceived by participants such as (spine-related, cardiovascular, neurological, or pulmonary disorders).
Procedure
During their initial visit to the outpatient physical therapy departments, participants with upper extremity musculoskeletal disorders were asked to complete the Arabic versions of the UEFI ( Aljathlani et al., 2022), and numeric pain rating scale (NPRS) ( Alghadir et al., 2016). In the same assessment session, general information about the participants was collected along with anthropometric data such as height and weight in order to provide clear descriptive statistics of the characteristics of the participants in the current study.
Outcome measures
UEFI
The UEFI is an upper extremity-specific outcome measure evaluating participants’ self-reported activity limitations across 20 items ( Stratford et al., 2001; Chesworth et al., 2014). Ratings for each item were assigned on a scale from 0 (representing extreme difficulty or an inability to perform the activity) to 4 (indicating no difficulty), with the total score derived from the summation of all item scores. The overall score for the UEFI ranges from 0 (reflecting the worst upper extremity function) to 80 (indicating the best upper extremity function). Previous research studies have established the construct validity, reliability, and responsiveness of the Arabic version of the UEFI utilized in the current study in patients with upper extremity musculoskeletal disorders ( Aljathlani et al., 2022; Alnahdi, 2023).
Numeric pain rating scale
The NPRS was employed to assess the average pain intensity experienced by the participant at the location of upper extremity dysfunction ( Hawker et al., 2011). Scores on the NPRS ranged from 0, indicating no pain, to 10, signifying the most severe pain imaginable. Earlier research studies have validated the measurement properties of the Arabic version of the NPRS in patients with musculoskeletal disorders including those with upper extremity disorders ( Alghadir et al., 2016; Alnahdi, 2021).
Statistical analysis
Structural validity of the Arabic UEFI was examined in the current study using EFA and CFA. The underlying structure of the Arabic UEFI was hypothesized to be unidimensional. This was based on the argument that all items measure one construct that is the level of upper extremity function and that all items are indicators of this one construct. In the EFA, factor extraction was conducted using the maximum likelihood method. The number of factors to be retained in the EFA was determined using parallel analysis where only factors with eigenvalue larger than the 95th percentile of the random data eigenvalue were retained ( O’Connor, 2000). Items’ factor loadings of at least 0.32 were considered the least magnitude, which indicates meaningful association between the item and factor ( Tabachnick and Fidell, 2013). The EFA and parallel analysis were conducted in the current research study using IBM SPSS Statistics 26 (IBM Corp., Armonk, NY, USA) and JASP (version 0.18.1.0).
Following EFA, the fit of the underlying structure identified using the EFA was examined using a CFA. Prior to conducting the CFA, evaluations for univariate and multivariate normality were performed, along with outlier detection. Chi-square statistic (χ 2) was used to assess model fit, with a nonsignificant result indicating a perfect fit. The χ 2 statistic was interpreted considering its known sensitivity to large sample sizes leading to indication of lack of good fit even when the data reasonably fit the model ( Byrne, 2010; Cappelleri et al., 2013) Other fit indices, such as the χ 2/degrees of freedom, the comparative fit index (CFI), the Tucker–Lewis index (TLI), the root mean square error of approximation (RMSEA), and the standardized root mean residual (SRMR), were used to assess model fit. The following cutoff values were used as indicators of good model fit: χ 2/df <3, CFI and TLI of at least 0.90 or above, RMSEA of 0.06 or below, and SRMR of 0.08 or below ( Hu and Bentler, 1999; Jackson et al., 2009). The UEFI data used in the current study had no missing items; thus, no imputations were performed. The CFA utilized maximum likelihood estimation through IBM SPSS AMOS (version 26, IBM Corp., Armonk, NY, USA). To identify model misspecifications, standardized residuals and modification indices (MI) were examined ( Byrne, 2010; Brown, 2015). The assessment of MI and our theoretical understanding of the content of the item guided the post hoc modifications to the CFA model.
Sample size estimation
As per the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN), a sample size that includes seven participants per scale item was rated as a very good sample size for the examination of structural validity of a PROM ( Mokkink et al., 2018). Accordingly, in alignment with the COSMIN guidelines, a sample size of 140 participants (7 participants for each of the 20 UEFI items) was deemed as the minimum required sample size for our specific objectives. The number of participants in the current study exceeded this minimum required sample size.
RESULTS
This study involved the participation of 256 individuals with upper extremity musculoskeletal disorders with characteristics detailed in Table 1. The majority of the participants exhibited dysfunctions in the shoulder and arm area, then wrist and hand, and finally disorders at the elbow and forearm. None of the participants had any missing items in the UEFI and other outcomes. Descriptive statistics of the UEFI items are included in Table 2.
Characteristics of participants ( N = 256).
| Variable | Mean ± SD or N (%) |
|---|---|
| Age (year) | 39.26 ± 14.02 |
| Sex | |
| Male | 146 (57.0) |
| Female | 110 (43.0) |
| Height (m) | 1.67 ± 0.09 |
| Mass (kg) | 76.24 ± 16.49 |
| Body mass index (kg/m 2) | 27.45 ± 5.64 |
| Site of dysfunction | |
| Shoulder and arm | 135 (52.7) |
| Elbow and forearm | 38 (14.8) |
| Wrist and hand | 83 (32.4) |
| Upper extremity surgery | |
| Yes | 100 (39.1) |
| Time after surgery (months) | 1.84 (2.07) * |
| No | 156 (60.9) |
| Duration of symptoms (months) | 2.99 (8.45) * |
| UEFI (0-80) | 44.26 ± 19.19 |
| NPRS (0-10) | 4.80 ± 2.35 |
Abbreviations: NPRS, numeric pain rating scale; SD, standard deviation; UEFI, upper extremity functional index.
*Median (interquartile range).
UEFI items’ statistics and EFA factor loading.
| Item | Mean | SD | Factor loading | % Floor | % Ceiling |
|---|---|---|---|---|---|
| 1. Any of your usual work, housework, or school activities | 2.18 | 1.02 | 0.72 | 7.0 | 8.2 |
| 2. Your usual hobbies, recreational or sporting activities | 1.75 | 1.21 | 0.51 | 18.8 | 7.4 |
| 3. Lifting a bag of groceries to waist level | 1.89 | 1.24 | 0.68 | 16.4 | 12.1 |
| 4. Placing an object onto, or removing it from an overhead shelf | 1.51 | 1.21 | 0.66 | 24.2 | 7.4 |
| 5. Washing your hair or scalp | 2.22 | 1.34 | 0.77 | 13.3 | 23.4 |
| 6. Pushing up on your hands (e.g. from bathtub or chair) | 2.09 | 1.34 | 0.75 | 18.0 | 18.0 |
| 7. Preparing food (e.g. peeling, cutting) | 2.33 | 1.37 | 0.81 | 13.7 | 26.2 |
| 8. Driving | 2.40 | 1.21 | 0.79 | 7.0 | 23.0 |
| 9. Vacuuming, sweeping, or raking | 2.23 | 1.32 | 0.82 | 13.7 | 21.5 |
| 10. Dressing | 2.50 | 1.20 | 0.78 | 6.3 | 27.0 |
| 11. Doing up buttons | 2.66 | 1.33 | 0.77 | 9.0 | 37.5 |
| 12. Using tools or appliances | 2.60 | 1.17 | 0.81 | 6.3 | 26.6 |
| 13. Opening doors | 2.71 | 1.22 | 0.74 | 5.9 | 35.5 |
| 14. Cleaning | 2.32 | 1.30 | 0.84 | 10.9 | 23.8 |
| 15. Tying or lacing shoes | 2.55 | 1.39 | 0.83 | 10.5 | 37.1 |
| 16. Sleeping | 2.33 | 1.23 | 0.51 | 8.2 | 21.5 |
| 17. Laundering clothes (e.g. washing, ironing, folding) | 2.20 | 1.39 | 0.85 | 16.0 | 24.6 |
| 18. Opening a jar | 1.96 | 1.36 | 0.77 | 18.4 | 16.4 |
| 19. Throwing a ball | 1.88 | 1.32 | 0.64 | 18.8 | 14.8 |
| 20. Carrying a small suitcase with your affected limb | 1.95 | 1.28 | 0.67 | 17.2 | 13.7 |
Abbreviations: EFA, exploratory factor analysis; SD, standard deviation; UEFI, upper extremity functional index.
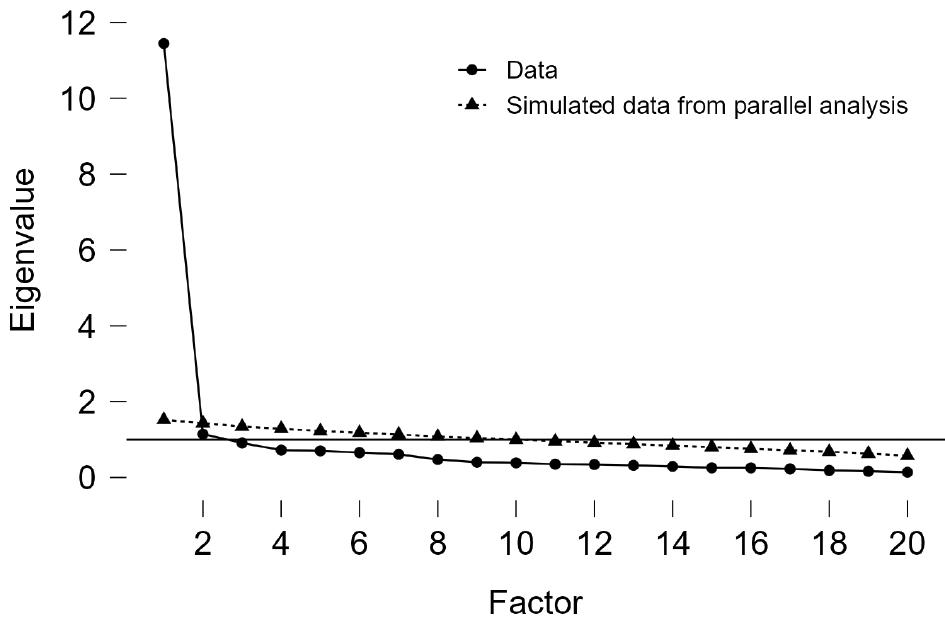
The Kaiser–Meyer–Olkin Measure of Sampling Adequacy registered a value of 0.95, and Bartlett’s Test of Sphericity showed significance ( P < 0.001), affirming the adequacy of the sample and appropriateness of the data for factor analysis. Parallel analysis revealed that only a single factor possessed an eigenvalue surpassing the random data eigenvalue ( Fig. 1). This observation implies that the Arabic UEFI exhibits a singular underlying factor structure reflecting upper extremity function, thereby endorsing the scale structural validity as a unidimensional measure. Based on the results of the parallel analysis, only one factor was extracted in the EFA of the Arabic UEFI accounting for 57.22% of the total variance that is 10 times the variance explained by the second factor ( Table 3). All the UEFI items showed substantial loadings on the single extracted factor with loadings ranging from 0.51 (item 2) to 0.85 (item 17) ( Table 2).
UEFI EFA factor structure.
| Factor | Initial eigenvalues | ||
|---|---|---|---|
| Total | % of Variance | Cumulative % | |
| 1 | 11.44 | 57.22 | 57.22 |
| 2 | 1.14 | 5.72 | 62.94 |
| 3 | 0.91 | 4.55 | 67.49 |
| 4 | 0.72 | 3.62 | 71.11 |
| 5 | 0.70 | 3.52 | 74.62 |
| 6 | 0.66 | 3.29 | 77.91 |
| 7 | 0.61 | 3.07 | 80.98 |
| 8 | 0.48 | 2.38 | 83.36 |
| 9 | 0.40 | 2.02 | 85.38 |
| 10 | 0.39 | 1.94 | 87.32 |
| 11 | 0.35 | 1.76 | 89.08 |
| 12 | 0.34 | 1.71 | 90.79 |
| 13 | 0.32 | 1.60 | 92.39 |
| 14 | 0.29 | 1.46 | 93.84 |
| 15 | 0.26 | 1.28 | 95.12 |
| 16 | 0.26 | 1.27 | 96.40 |
| 17 | 0.228 | 1.14 | 97.54 |
| 18 | 0.187 | 0.94 | 98.47 |
| 19 | 0.166 | 0.83 | 99.30 |
| 20 | 0.139 | 0.70 | 100.00 |
Abbreviations: EFA, exploratory factor analysis; UEFI, upper extremity functional index.
The initial CFA model that was examined included one latent variable (upper extremity function) and 20 indicators (UEFI items) and resulted in the following fit indices: χ 2 = 624.84 (df = 170, P < 0.001), χ 2/df = 3.68, TLI = 0.87, CFI = 0.88, RMSEA = 0.10 (90% CI = 0.09-0.11), and SRMR = 0.051. These fit indices did not support the fit of the data to the proposed unidimensional model. The examination of MI in the initial CFA model revealed areas of model misfit including high error covariance between items representing similar tasks. These high error covariances were observed between the following items: items 1 and 2; items 3 and 4; items 4 and 5; items 3 and 20; items 7 and 18; items 9 and 17; items 10 and 11; and items 11 and 15. Allowing these error terms to covary ( Fig. 2) improved the fit of the modified model and resulted in the following fit indices: χ 2 = 665.94 (df = 162, P < 0.001), χ 2/df = 2.88, TLI = 0.91, CFI = 0.92, RMSEA = 0.086 (90% CI = 0.077-0.095), and SRMR = 0.045. These model fit indices suggested acceptable fit of the data to the modified model ( Fig. 2). Parameter estimates including unstandardized and standardized estimates for the final CFA model are shown in Table 4. Each of the UEFI items displayed significant positive loading in accordance with the anticipated correlation pattern between the single latent variable representing upper extremity function and the UEFI items ( Table 4).
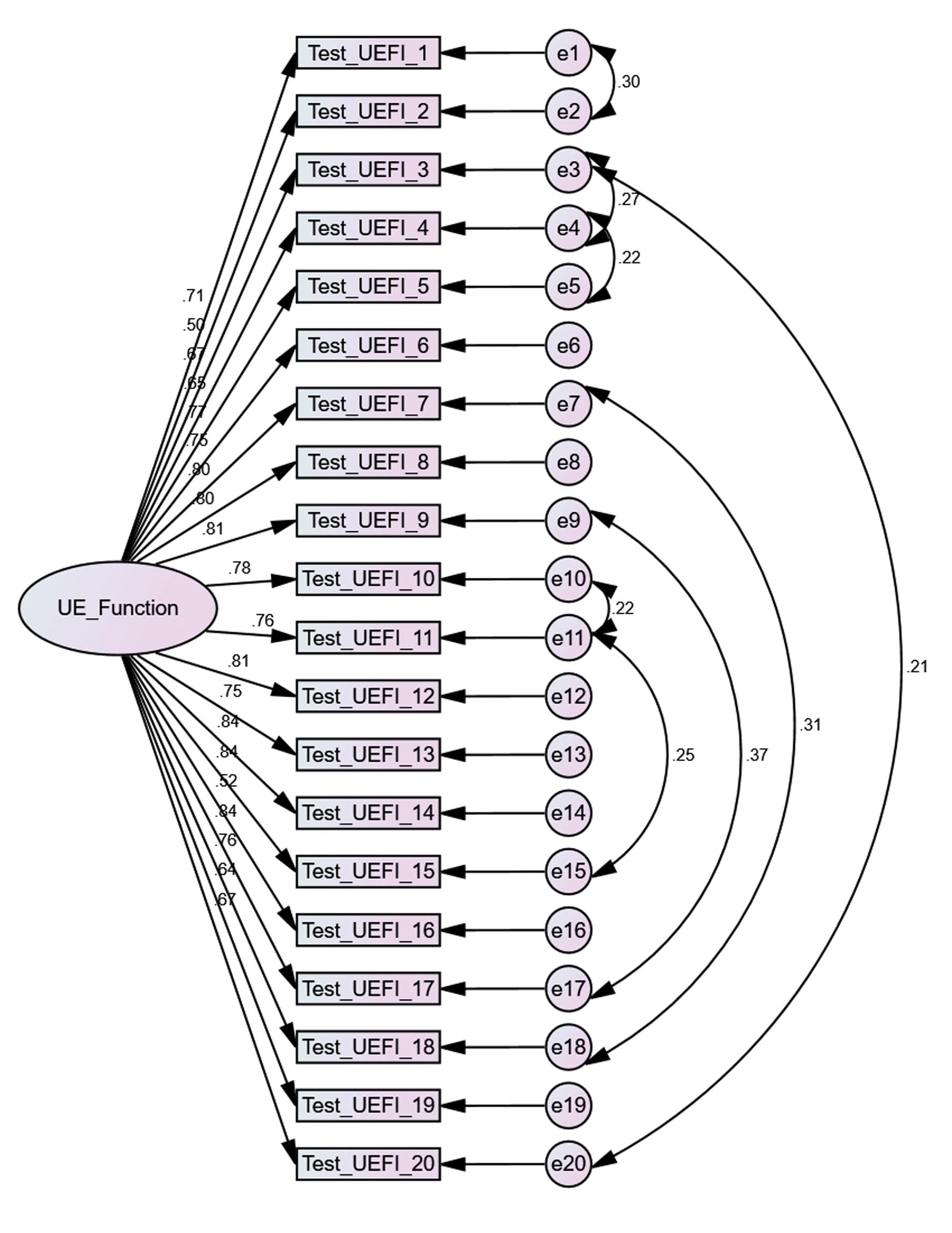
The final confirmatory factor analysis model that showed adequate model fit. Abbreviation: UEFI, upper extremity functional index.
Confirmatory factor analysis parameter estimates.
| UEFI items | Standardized loading | Unstandardized loading | SE | CR | P |
|---|---|---|---|---|---|
| 1. Any of your usual work, housework, or school activities | 0.72 | 1.00 a | — | — | — |
| 2. Your usual hobbies, recreational or sporting activities | 0.50 | 0.83 | 0.09 | 9.04 | <0.001 |
| 3. Lifting a bag of groceries to waist level | 0.67 | 1.14 | 0.11 | 10.55 | <0.001 |
| 4. Placing an object onto, or removing it from an overhead shelf | 0.65 | 1.08 | 0.11 | 10.20 | <0.001 |
| 5. Washing your hair or scalp | 0.77 | 1.42 | 0.12 | 12.09 | <0.001 |
| 6. Pushing up on your hands (e.g. from bathtub or chair) | 0.75 | 1.37 | 0.12 | 11.77 | <0.001 |
| 7. Preparing food (e.g. peeling, cutting) | 0.80 | 1.51 | 0.12 | 12.60 | <0.001 |
| 8. Driving | 0.80 | 1.33 | 0.11 | 12.61 | <0.001 |
| 9. Vacuuming, sweeping, or raking | 0.81 | 1.46 | 0.12 | 12.78 | <0.001 |
| 10. Dressing | 0.78 | 1.29 | 0.11 | 12.36 | <0.001 |
| 11. Doing up buttons | 0.76 | 1.39 | 0.12 | 11.97 | <0.001 |
| 12. Using tools or appliances | 0.81 | 1.31 | 0.10 | 12.82 | <0.001 |
| 13. Opening doors | 0.75 | 1.27 | 0.11 | 11.89 | <0.001 |
| 14. Cleaning | 0.85 | 1.51 | 0.11 | 13.38 | <0.001 |
| 15. Tying or lacing shoes | 0.84 | 1.60 | 0.12 | 13.22 | <0.001 |
| 16. Sleeping | 0.52 | 0.87 | 0.11 | 8.09 | <0.001 |
| 17. Laundering clothes (e.g. washing, ironing, folding) | 0.84 | 1.60 | 0.12 | 13.28 | <0.001 |
| 18. Opening a jar | 0.76 | 1.42 | 0.12 | 11.97 | <0.001 |
| 19. Throwing a ball | 0.64 | 1.16 | 0.12 | 10.03 | <0.001 |
| 20. Carrying a small suitcase with your affected limb | 0.67 | 1.18 | 0.11 | 10.49 | <0.001 |
Abbreviations: CR, critical ratio; UEFI, upper extremity functional index; SE, standard error.
aThis factor loading was fixed to 1 and thereby had no associated standard error, critical ratio, or P value.
DISCUSSION
This research study was conducted to examine the structural validity of the Arabic UEFI using both EFA and CFA in patients with upper extremity musculoskeletal disorders. The current study is the first and only study that examined the structural validity of the Arabic UEFI. We hypothesized that the Arabic UEFI would demonstrate a unidimensional structure reflecting one latent variable that is upper extremity function. The results of the EFA supported this hypothesized unidimensional structure while the CFA supported this hypothesized unidimensional structure after accounting for possible response dependency among some of the items.
The UEFI was developed as a unidimensional structure measuring one latent construct that is upper extremity function. The results of the EFA supported our hypothesized unidimensional structure. The method used in the current study to determine the number of factors to be extracted in the EFA was the parallel analysis. This method of determining the number of factors is believed to be the more objective method compared to the other methods of determining the number of factors such as eigenvalue >1 or visual examination of the scree plot ( Cappelleri et al., 2013).
In the original development of the UEFI, EFA was used for reducing the number of items to be included in the scale, but the details and results of factor analysis for the final 20 items of the UEFI were not reported by the original developers of the scale ( Stratford et al., 2001). Similarly, the available studies that examined the measurement properties of the UEFI in patients with upper extremity musculoskeletal disorders including the Turkish ( Aytar et al., 2015), Greek ( Karanasios et al., 2023) and Chinese ( Xiao et al., 2012) versions did not examine the scale structural validity. Additionally, Binkley et al. examined the measurement properties of the UEFI in patients with breast cancer paper of UEFI but failed to examine the scale structural validity using either EFA or CFA ( Binkley et al., 2018). Based on that, the results presented in the current study regarding the structural validity of the UEFI using EFA or CFA could not be compared to other similar previous studies given the lack of structural validity assessment in these studies or any other studies in the literature.
Structural validity assessment has been reported for the Chinese 15-item UEFI, reduced version of the 20-item UEFI, in patients with stroke ( Pan et al., 2023). The authors used principal component analysis with scree plot assessment for determining the number of factors within the scale and used the oblique promax rotation. The authors suggested that the 15-item Chinese UEFI has a two-dimensional structure representing basic daily activity and advanced functional activity ( Pan et al., 2023). The two-dimensional structure suggested by the EFA in the Chinese version contradicts the findings of the EFA in the current study that suggest a unidimensional structure for the 20-item UEFI. This contradiction could be attributed to the use of the scree plot for determining the number of factors in the Chinese version where this method is known to be less than optimal compared to parallel analysis used in the current study ( Cappelleri et al., 2013). We believe that the robust parallel analysis gives more credibility to the dimensionality findings in our study compared to that of the Chinese 15-item UEFI.
The initial analysis of the CFA model with 1 latent variable (upper extremity function) and 20 indicators (UEFI items) revealed model misfit suggesting deviations of the data from the specified unidimensional model. The main reason for the deviation from the specified unidimensional model was the high error covariance between items representing similar upper extremity function. These error terms were modeled initially without covariance among them based on the assumption that UEFI items are indicators of one latent variable (upper extremity function) and are influenced only by changes in this construct, and that the error terms represent random variance that is not explained by the latent variable. Based on that, the error terms that represent random variance were not expected to correlate.
The initial analysis did not support the unidimensionality of the UEFI. This lack of unidimensionality could be attributed to the presence of another latent variable or the presence of response dependency ( Tennant and Conaghan, 2007; Hagquist et al., 2009). The argument of the presence of another latent variable would suggest that the UEFI is a multidimensional measure where at least some of the scale items are systematically influenced by another latent variable representing another construct other than upper extremity function. The other argument that might explain the initial deviation from unidimensionality is the presence of response dependency among the UEFI items. The presence of response dependency would suggest that responses to items are not independent and that responses are linked for example because of similar content in these items.
Examining the content of the items that exhibited high error covariance would help in explaining this deviation from unidimensionality. Some of the item pairs with high MI associated with error covariance were item 4 (placing an object onto, or removing it from an overhead shelf) with item 5 (washing your hair or scalp); item 3 (lifting a bag of groceries to waist level) with item 20 (carrying a small suitcase with your affected limb); and item 11(doing up buttons) with item 15 (tying or lacing shoes). The items 4 and 5 represent similar upper extremity function that is arm elevation above the shoulder level. The items 3 and 20 also represent similar upper extremity function that is lifting and carrying where an object is held with one hand and then lifted. Moreover, items 11 and 15 also represent similar upper extremity function that require bimanual involvement with fine hand control. The same pattern was also observed for all item pairs with high error covariance where all of these item pairs reflected similar upper extremity functions. Overall, it seems that response dependency might provide a more plausible explanation of the lack of unidimensionality observed initially.
To the best of our knowledge, there is no study in the literature that examined the structural validity of the 20-item UEFI using CFA, with only one prior study that examined the structural validity of a 15-item UEFI using CFA. CFA has been conducted to examine the structural validity of the Chinese 15-item UEFI in patients with stroke ( Pan et al., 2023). The author examined the fit of a two-factor model (basic daily activity and advanced functional activity) identified earlier by the authors using principal component analysis. The authors suggested good fit to the two-factor model while the fit indices reported do not support the fit of the data to hypothesized two-factor model (CFI = 0.872, TLI = 0.849, and RMSEA = 0.113). The values of these fit indices did not reach thresholds commonly recommended for acceptable model fit.
Hamilton et al examined the dimensionality and structural validity of the UEFI using the Rasch measurement model ( Hamilton and Chesworth, 2013). The authors reported deviation of the 20-item UEFI from unidimensionality partly because of the observed residual correlation between item 11 (doing up buttons) with item 15 (tying or lacing shoes). This observed residual correlation is similar to the high error covariance observed in the current study supporting our argument of possible response dependency between these items of similar function. Hamilton et al. addressed this response dependency issue by deleting item 15 (tying or lacing shoes), while in the current study the issue of response dependency was accounted for by adding error covariance between items that represent somewhat similar upper extremity function.
The current study is not without limitations. Elbow and forearm disorders represent a small proportion of the participants; therefore, results should be interpreted with caution for patients with disorders in this region. Further analysis of the internal structure of the Arabic UEFI, including validity of the response options, measurement invariance, and transformation of the ordinal total score into interval-level score using the Rasch measurement model might be needed. On the other hand, the current study included excellent sample size that largely exceeded the number of participants recommended by COSMIN for examining a PROM structural validity with complete dataset and no imputations providing confidence in the results obtained. The outcome of the current study would allow the use of the Arabic UEFI in daily clinical practice and in research studies with greater confidence that the scale scoring method using one total score is valid for reflecting the construct measured by the scale that is upper extremity function.
CONCLUSION
This research study was conducted to examine the structural validity of the Arabic UEFI using both EFA and CFA in patients with upper extremity musculoskeletal disorders. The results of the EFA supported this unidimensional structure of the UEFI while the CFA supported this unidimensional structure after accounting for possible response dependency among some of the items.