
Introduction
Fulminant myocarditis (FM), a type of acute myocarditis, leads to a rapid progressive decline in cardiac function, characterized by sudden and severe diffuse inflammation of the heart, and often leading to cardiogenic shock, ventricular arrhythmias, multi-organ system failure, and death. FM usually occurs within 2 to 3 days after precursor symptoms, such as fatigue, cough, and dyspnea, and progresses within 2 weeks to severe left ventricular systolic dysfunction, hemodynamic dysfunction, and circulatory instability requiring positive inotropic medication and/or mechanical circulatory support [1]. The annual incidence of various types of acute myocarditis ranges from 0.22% to 1.14% [2–4]. FM is rare, accounting for about 2.5% of cases of acute myocarditis but about 30% of hospitalisations for myocarditis, and has a higher mortality rate and poorer long-term prognosis than other types of myocarditis. The cumulative risk of death or heart transplantation within 30 and 90 days is 22% and 29%, respectively. The cumulative risk of death or heart transplantation after 7 years of follow-up in patients with FM is 47.7%. The mechanisms underlying the long-term pathophysiological prognosis of patients with myocarditis remain unclear. More than 20% of patients with FM have been reported to have heart failure, arrhythmias, or cardiomegaly at 1-year follow-up [5]. These findings suggest that FM requires long-term follow-up and management. However, diagnostic and follow-up methods are lacking in patients with FM. Endomyocardial biopsy is not commonly used clinically, because of its adverse effects, and need for specialized personnel and equipment. Cardiac magnetic resonance (CMR) is a time-consuming and artifact-prone procedure that has limitations in clinical use [6].
Optical pumped magnetometer magnetocardiography (OPM-MCG) can simultaneously detect and record magnetic field signals in 36 locations on the chest of a patient. This method, with a magnetic field detector and analysis software, can create a real-time magnetic field map, pseudo current density map, and MCG waveforms. MCG has higher diagnostic accuracy and sensitivity for CAD compared to ECG [7–9]. It is also effective in diagnosing patients with NSTEMI and detecting myocardial ischaemia as defined by FFR [10–11]. This article presents the case of a patient with FM who was diagnosed and monitored with OPM-MCG. This method may provide new options for managing patients with FM. The patient provided signed informed consent.
Case
A 37-year-old man was admitted to our hospital with intermittent chest tightness over the prior 4 days. He had fainted once after experiencing the symptom, but he regained consciousness spontaneously within several seconds, and had normal speech and movement of limbs. Two days before admission, he developed fever, cough, weakness, and sweating. His active tolerance function assessment was approximately 1 metabolic equivalent (MET). There was no documented personal or familial medical history of cardiac or cerebrovascular disease. The patient’s blood pressure reading was 100/53 mmHg. The ECG revealed low voltage in the extremity leads, a flattened T wave, avL and V1 in QS type, right deviation of the electrocardiographic axis, no discernible abnormalities in the ST segment, and a non-infarctive Q wave, indicating potential myocardial cell injury (Figure 1). The patient had a serum troponin I (hs TnI) level of 5103.5 pg/mL, B-type urinary natriuretic peptide (BNP) level of 1114.0 pg/mL, and N-terminal-B-type natriuretic peptide precursor (NT-proBNP) level of 21,825.00 pg/mL. Additionally, he tested positive for IgG antibodies to novel coronavirus, anti-CMV IgG, VCA IgG, EBNA IgG, and anti-B19 IgG. Echocardiography revealed a left ventricular ejection fraction (EF) of 39%, an interventricular septum thickness of 15 mm, and a left ventricular end-diastolic internal diameter (LVDd) of 44 mm. The OPM-MCG results exhibited several anomalies, such as a magnetic field deflection angle exceeding 45° in a clockwise direction, irregularities in the distribution of positive poles, and anomalies in the characteristic parameters (Table 1). Concurrently, the patient demonstrated a peak R amplitude of 30 PT (Figure 2B). He then underwent CMR, with T2 images showing high signal in the left ventricular myocardium suggestive of extensive myocardial edema (Figure 3A). Invasive coronary angiography revealed a myocardial bridge (MB) in the middle of the left anterior descending branch, with a systolic compression ratio of 90%, and TIMI flow grade III. On the basis of these clinical findings, the patient was diagnosed with FM, heart failure with reduced ejection fraction, and MB. The patient underwent immunomodulatory therapy with methylprednisolone sodium succinate; anti-infective therapy with oseltamivir; anti-heart failure therapy with sacubitril valsartan and torasemide; and myocardial trophic therapy with vitamin C, sodium fructose diphosphate, and coenzyme Q10. His symptoms and laboratory parameters significantly improved before hospital discharge (Table 2).
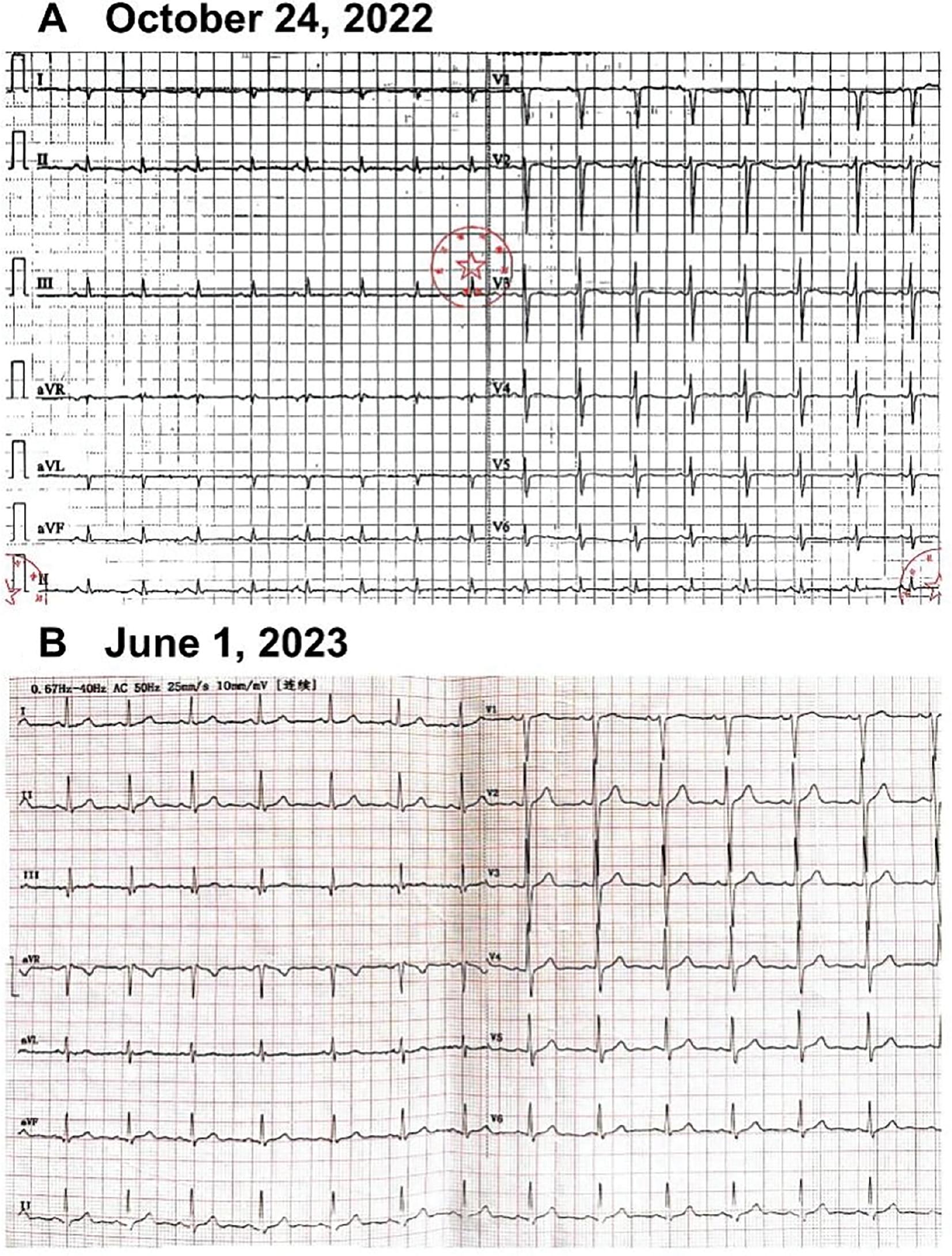
ECG on October 24, 2022, and June 1, 2023.
(A) ECG on October 24, 2022, showed low voltage and a flattened T-wave in the limb leads, avL and V1 in QS type, right deviation of the electrocardiographic axis, and no discernible abnormalities in the ST segment. (B) ECG on June 1, 2023, was normal. ECG (electrocardiogram).
MCG Parameters.
| Examination time | MAg-Tp | RtoAm-Tp | MAgmax-TT | MAgmin-TT | CAgmax-Tp | δAgmax-C | δAgmin-C | MAg-RpTp |
|---|---|---|---|---|---|---|---|---|
| Reference value | −86°~45° | 0.3~0.9 | −98°~−33° | −85°~−50° | −5−77° | −10−80° | −20−60° | 0.1~0.66 |
| October 27, 2022 | 2.24° | 0.54 | −2.52° | −23.07° | 86.42° | 87.86° | 77.52° | 0.37 |
| June 1, 2023 | −67.17° | 0.54 | −67.17° | −72.70° | 32.49° | 87.86° | 32.49° | 0.32 |
M: Magnetic Field; Ag: Angle; Tp: T-peak; Rto: Ratio; Am: Amplitude; max: Maximum; C: Current; δ: Change value; min: Minimum; Rp: R-peak.
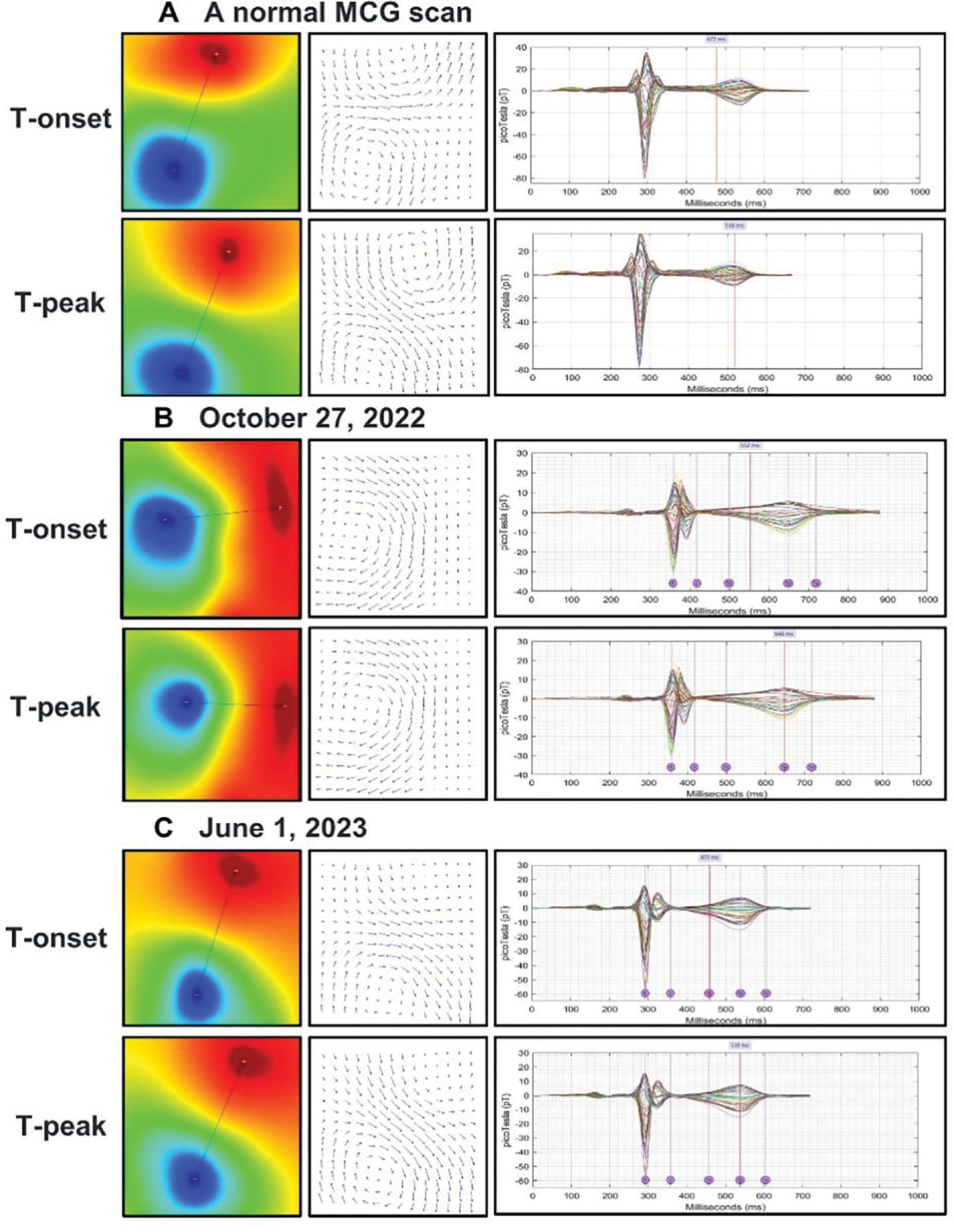
A Normal OPM-MCG, and the Patient’s OPM-MCG Scans on October 27, 2022, and June 1, 2023.
(A) A normal OPM-MCG scan showed no evidence of myocardial injury or obstructive coronary artery disease, as demonstrated by the lack of significant current deviations within the myocardium, and an absence of angle shift (indicated by black arrow) between the positive red pole and negative blue pole between the T wave onset (T-onset) and T wave peak (T-peak). (B) An abnormal OPM-MCG scan on October 27, 2022, showed a magnetic field deflection angle exceeding 45° in the clockwise direction (indicated by black arrow), irregularities in the distribution of positive poles at T-onset and T-peak. (C) During the 7-month follow-up, OPM-MCG showed no clear abnormalities. OPM-MCG (optical pumped magnetometer magnetocardiography), T-onset (onset of the T wave), T-peak (peak of the T wave).
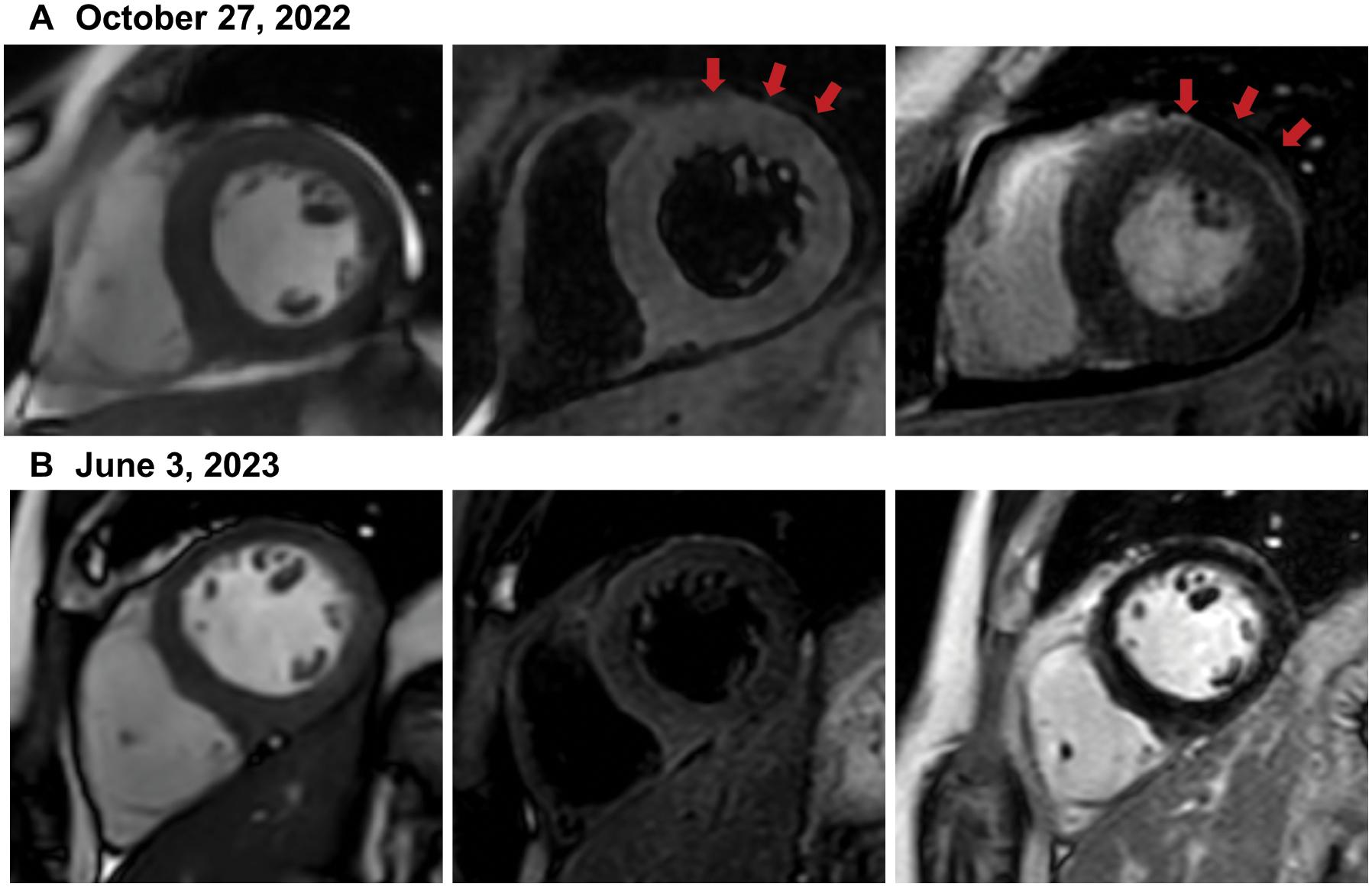
CMRs on October 27, 2022, and June 3, 2023.
The CMRs depict the central segment of the left ventricle of the patient on October 27, 2022, and June 3, 2023. The images showing the cine sequence, T2 sequence, and late gadolinium enhancement, arranged from left to right, revealed notable changes over time. (A) On October 27, 2022, CMRs at the level of the papillary muscles, the patient exhibited a high signal in the ventricular myocardium on T2-weighted imaging, along with multiple patches of slightly high signal on gadolinium enhancement, indicative of myocardial edema. (B) On June 3, 2023, CMRs at the level of the papillary muscles, a significant decrease in myocardial edema was observed with respect to the prior imaging session. CMR (cardiac magnetic resonance).
Laboratory and Echocardiography Results.
| Reference | October 24, 2022 | October 31, 2022 | June 1, 2023 | |
|---|---|---|---|---|
| Admission laboratory results | ||||
| CRP (mg/L) | 0–8 | 42.66 | 1.64 | 1.26 |
| WBC (×109/L) | 3.5–9.5 | 14.09 | 11.98 | 6.72 |
| LYM (%) | 20–50 | 11.5 | 23.8 | 29.8 |
| NE (%) WBC | 40–75 | 74.1 | 53.1 | 57.8 |
| RBC (×1012/L) | 4.3–5.8 | 5.04 | 4.85 | 5.02 |
| Hb (g/L) | 130–175 | 152 | 149 | 156 |
| PLT (×109/L) | 125–350 | 291 | 278 | 262 |
| hs TnI (pg/mL) | 0–19.8 | 5103.5 | 127.6 | 5.5 |
| BNP | 0–100 | 1114 | 9 | |
| NT-proBNP (pg/mL) | <300 | 21,825.00 | 312.00 | |
| Echocardiography results | ||||
| EF (%) | 39 | 60 | 62 | |
| IVS thickness (mm) | 15 | <12 | 9 | |
| LVDd (mm) | 44 | 49 | 45 | |
CRP: rapid C-reactive protein; WBC: white blood cell; LYM: lymphocyte; NE: neutrophilic granulocyte; RBC: red blood cell; Hb: hemoglobin; PLT: platelet; hs TnI: high-sensitivity troponin-I; BNP: brain natriuretic peptide; EF: ejection fraction; IVS: interventricular septum; LVDd: left ventricular end-diastolic internal diameter.
Follow-up
During the 7-month follow-up, the patient had no chest discomfort. His active tolerance function assessment was >10 METs. His blood count and inflammatory markers were normal: hs TnI = 5.5 pg/mL, BNP = 9 pg/mL (Table 2). Echocardiography revealed that the left ventricular EF was 62%, the thickness of the interventricular septum was 9 mm, and the end-diastolic internal diameter of the left ventricle was 45 mm. Reexamination of the OPM-MCG showed no clear abnormalities (Figure 2C). The amplitude of the R peak increased significantly, to 60 pt, and the characteristic parameters of the cardiac magnetic map were essentially normal (Table 1). CMR on June 1, 2023 indicated essentially normal findings (Figure 3B).
Discussion
MCG Imaging in Patients with FM
Cardiomyocytes communicate through electrical signals that create weak magnetic fields in the heart. With optical pumped magnetometers, data can be recorded at 36 positions in 90 seconds to create a two-dimensional magnetic field map, pseudo current density map, and MCG waveform. The TT segment, representing the time interval of myocardial repolarization, is often used in studies to analyze MCG images for both qualitative and quantitative purposes [12, 13]. In normal MCGs, the magnetic field map and pseudo current density map remain stable from the start of the T-onset to the T-peak. Furthermore, in accordance with Ampere’s law and the orientation of the cardiac electrical activity vectors, the orientation of the magnetic field vectors during the cardiac repolarization phase is 86° to 45°. In cases of myocardial cell injury, the conduction of myocardial action potentials is hindered, thus resulting in pathological irregularities in the depolarization and repolarization processes within the affected area and its vicinity. Localized damage to the heart affects myocardial currents, as seen on MCG images as changes in the magnetic field map and pseudo-current density map on the TT segment (from T-onset to T-peak). These changes are reflected by variations in the dipole, current angle, and magnetic angle. Furthermore, a correlation was found between the amplitude of the R-peak and cardiac function at the study center, thus indicating an association between decreased R-peak amplitude and heart failure.
On the basis of these principles, MCG exhibits high sensitivity in the identification of cardiomyocyte injury, even in asymptomatic or atypically presenting cases. This imaging technique may provide crucial early diagnostic data for the treatment of FM. The MCG results for our patient with FM corresponded to the typical abnormalities detected in MCGs and suggested the development of myocardial injury. The patient displayed initial disease manifestations, such as magnetic field angle deviation, anomalous positive pole distribution, and parameter abnormalities, in line with his clinical presentation. After 7 months, his MCG parameters returned to normal, and magnetic field map and pseudo current density map revealed no notable irregularities in the TT segment.
The Value of MCG Applications in FM
FM has rapid progression and poor prognosis. Early diagnosis is key, but endomyocardial biopsy, the preferred method, it is not always accessible. Clinical symptoms and CMR are often used for diagnosis, but can be expensive and time-consuming. Non-invasive methods, such as ECG, have limitations due to tissue conduction and a limited number of leads. Tolstrup et al. [14] have found that MCG is more sensitive and accurate than ECG when combined with troponin and either invasive coronary angiography or SPECT for detecting myocardial injury. The results in our case showed that MCG can provide clinical evidence of myocardial injury in the early stages of the onset of FM. Moreover, the MCG findings showed high concordance with the recovery of exercise tolerance, cardiac function, and nuclear magnetic resonance at the 7-month follow-up. These findings support MCGs potential to provide valuable clinical information regarding early myocardial damage in FM and to facilitate ongoing monitoring.
Magnetocardiography has shown promise in assessing myocardial injury in studies using various parameters to diagnose cardiovascular diseases. Lim et al. [15] have found that MCG has high accuracy in diagnosing NSTEMI, with a sensitivity of 96.4% and specificity of 85%. Shin et al. [16] have found that combining quantitative and qualitative MCG parameters can accurately diagnose CAD in patients without typical angina with 84.8% accuracy. However, current MCG technology cannot visually identify the cause of myocardial injury. Future clinical studies and advanced analysis methods, such as machine learning, are needed to improve MCG’s diagnostic capabilities.
MCG for Evaluating Treatment Options for Patients with MB
Our findings indicate that MCG may be a valuable tool for assessing treatment strategies for MB, a congenital anomaly in which a coronary artery courses through the myocardium and is present in approximately one-third of adults [17]. The treatment of asymptomatic patients is generally not advised, whereas cardiac surgery may be a viable option for individuals with refractory angina. Patient-reported symptoms are often subjective in nature, and definitive guidelines or clinical trials are lacking for the pre-surgical evaluation of patients with MB [18]. In the case, patient exhibited a systolic compression ratio of 90% in the left anterior descending MB. However, after complete recovery from FM, no significant positive findings were detected on the MCGs, suggesting that the myocardial bridge did not lead to myocardial injury. Consequently, MB interventions were not deemed necessary for our patient. Overall, OPM-MCG has the potential to evaluate the severity of MB in patients, because myocardial ischemia resulting from MBs may manifest as abnormalities in the TT segment of the MCGs. Consequently, OPM-MCG may serve as a tool for assessing myocardial ischemia induced by MB, thereby providing clinical guidance regarding the need for intervention.
Conclusion
OPM-MCG is a valuable tool for therapy monitoring in FMs, serving as a safe, non-invasive, and highly effective test for ancillary diagnostics and long-term prognostic follow-up. Additionally, MCG may aid in clinical decision-making regarding the need for further interventions in patients with MB.